F Rubba, S Campanile, C Viscardi, P Riccio, A Carnimeo, A Bosco, CM Mendillo, E Cascone, R Montalti, P Montuori, E Bianco R Troisi
“Did you hear me? A hospital without water supply, the maternity ward next to the infectious diseases ward. I refused to work for hell” W Marasco – With my back to this world, 2025
The present work arises from the need to observe the operating block not only as a technical place of the surgical act, but as a dynamic system of relationships, crossed by flows, interactions and invisible vulnerabilities that directly affect patient safety. The main objective was to analyze, from an organizational and structural perspective, the internal pathways within the operating block, with particular attention to the prevention of healthcare-associated infections (HAIs) in the patient undergoing kidney transplantation, a subject who by definition presents a condition of high immunological fragility [1,11]. The study is articulated in two complementary dimensions:
The observational component was based on a descriptive analysis of the organization of spaces, care pathways and flows of patients, operators and materials. Such analysis was conducted through the systematic study of floor plans and of the available organizational and regulatory documentation [6], allowing the reconstruction of the theoretical structure of the pathways and its comparison with the real layout;
The experimental component, of a non-interventional nature, instead concerned the identification of critical interferences between flows and the development of proposals for organizational and procedural improvement. The objective was not to modify the existing architectural layout, but rather to identify compensatory measures consistent with current regulations and with best practices in infection risk prevention [1,4].
This integrated approach made it possible to combine the systematic observation of the real context with an application-oriented reflection aimed at continuous improvement, strengthening the perspective of safety governance and promoting an organizational model based on critical analysis of processes and optimization of care pathways [16].
The study was conducted at the operating block of the University Hospital Federico II, with specific reference to Plate B of Building 5, an area dedicated to transplant activity. Plate B is part of a context of complex healthcare construction, characterized by the coexistence of operating rooms, filter areas, support rooms, administrative spaces and connecting corridors [15]. In this configuration, multiple types of flows converge and overlap: clinical, logistical, care-related.
Within the operating block there is also the presence of two distinct types of patients: on the one hand the patient candidate for transplant or already undergoing kidney transplant; on the other hand the dialysis patient who, for organizational and logistical needs, is directed to undergo treatment within the same block. This coexistence determines a significant management criticality, as both categories share common pathways and flows. The condition of immunodepression that characterizes the transplant patient gives this context particular relevance from the perspective of HAI risk [1,10,11]. The sharing of the same corridors and transit areas with dialysis patients can favor the onset of problems related to the management of cross infections, especially in the post-transplant phase [3]. In this scenario, every interference between pathways and every possible indirect contamination assume an amplified weight compared to other care settings, making careful organizational regulation of flows essential [8].
The analysis was developed through three main tools:
study of the floor plans of the operating block and Plate B;
analysis of regulatory and organizational documentation;
systematic mapping of internal flows.
Five main flows were identified:
flow of the patient undergoing organ transplant;
flow of the patient undergoing dialysis;
flow of healthcare personnel;
flow of clean materials;
flow of dirty materials.
The evaluation of infectious risk was developed through a systematic analysis based on structured criteria consistent with the principles of biological risk prevention [8]. In particular, attention focused on the type of flows involved, on the frequency and on the concrete modes of use of the pathways, as well as on the presence of possible interferences between clean and dirty flows. The probability of cross-contamination was also considered, evaluating to what extent the sharing of spaces could favor the indirect transfer of microorganisms through surfaces, devices, air or occasional contacts mediated by healthcare personnel [13]. A further element of analysis concerned the presence or absence of risk mitigation measures, such as filter zones, structural separations or specific organizational procedures [14]. The critical issues that emerged were then weighted and classified in relation to their potential impact on infectious risk, not in abstract terms, but in relation to patient vulnerability and to the concrete operativity of the context [1,11]. This classification constituted the basis for the development of targeted improvement proposals. Where structural intervention was not feasible, an organizational and procedural approach was preferred, particularly enhancing the temporal separation of flows as a compensatory measure capable of reducing interferences and strengthening the safety of care pathways without modifying the existing architectural layout [14].
The floor plan of Plate B returns the image of a complex architectural organism, in which each space responds to a function and each pathway translates an organizational principle. The structure develops along clearly defined circulation axes, which organize and connect two macro-areas functionally distinct but integrated into a single system. The distribution layout is not random, but responds to a design logic aimed at ensuring order, separation of pathways and coherence between function and space:
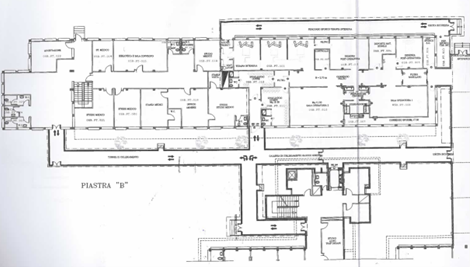
In the left portion of the floor plan is located the support and administrative area: medical offices, library, conference room, offices and reception outline a space dedicated to planning, comparison and management activities. These are environments characterized by a low bacterial load, physically separated from the surgical area, conceived to allow staff to carry out organizational and scientific functions without interfering with high-intensity clinical activities.
In the right portion, instead, the operational core of the block is concentrated: the operating rooms, protected by filter zones that regulate access and ensure decontamination, the intensive care area and the post-operative ward. Here space assumes an eminently clinical dimension, designed to accommodate the patient in the most critical phases of the care pathway. The functional contiguity between these environments is not only an architectural element, but a precise organizational choice: to reduce to a minimum the transfer times of the critical patient, ensure continuity of care and maintain conditions of maximum sterility along the entire intra-hospital path.
The color mapping made it possible to clearly distinguish the pathways.
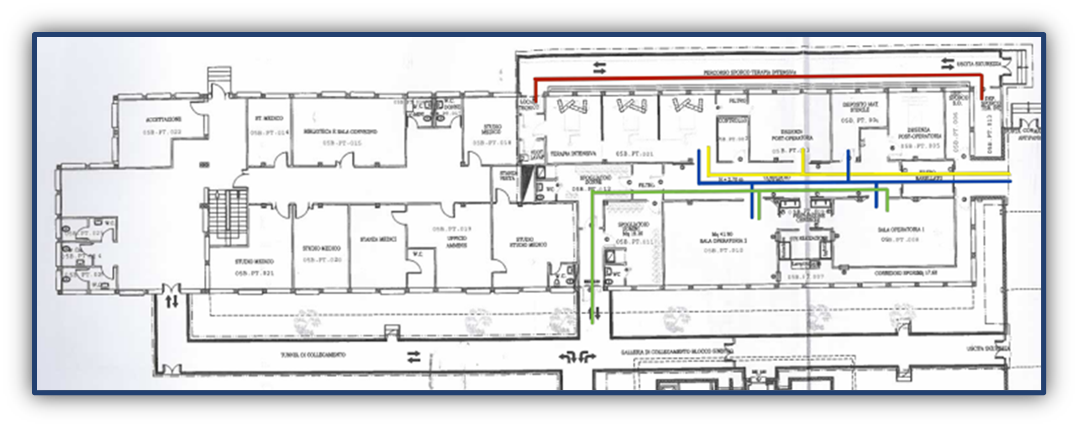
The dirty pathway (red line) develops along an external perimeter corridor, separated from sterile areas. It ensures the evacuation of biological waste, infected linen and instruments to be sterilized, in compliance with the principle of “forward movement”.
The clean pathway of operators (green line) requires mandatory passage through filter zones, changing rooms and surgical washing areas, ensuring that only adequately decontaminated personnel access critical areas.
The patient pathways are distinguished into:
transplant patient pathway (blue line), directed towards the operating room with maximum level of protection; dialysis patient pathway (yellow line), directed towards intensive care and nephrological support areas.
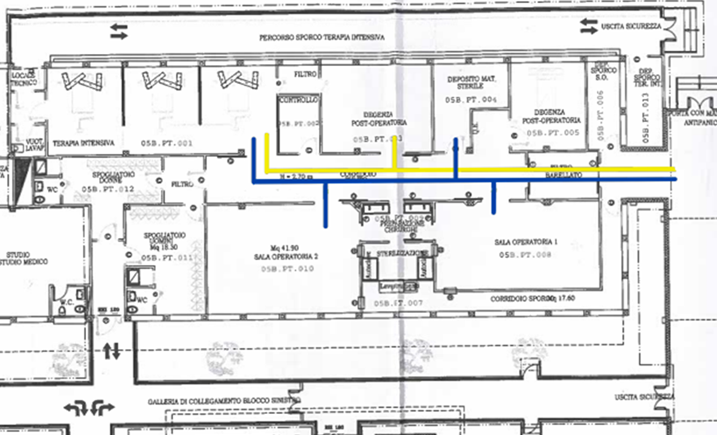
The analysis of pathways brought to light a structural criticality of particular relevance: the overlap between the route intended for the patient undergoing transplant and that reserved for the dialysis patient. Both flows start from the same filter area and continue along the same distribution corridor, determining a spatial continuity that, in fact, cancels the distinction between care pathways profoundly different in nature and level of vulnerability. This configuration interrupts the fundamental principle of separation of flows, cornerstone of the organization of high-complexity operating blocks. The sharing of spaces, in a context in which contamination control represents an absolute priority, introduces an element of systemic fragility. The transplant patient, especially in the perioperative phase, is in a condition of marked immunodepression, which makes them particularly susceptible even to minimal environmental exposures. At the same time, the dialysis patient constitutes a clinically complex population, frequently bearer of permanent vascular accesses and, not infrequently, of chronic infections or bacterial colonizations. The coexistence of such conditions along the same corridor amplifies the risk of indirect contamination, which can occur through surfaces, airborne micro-particles, medical devices or occasional contacts mediated by personnel. What emerges is an evident misalignment between the structural layout of spaces and the clinical-care needs specific to the transplant pathway: a discrepancy that does not limit itself to an architectural datum, but translates into an organizational vulnerability with potential repercussions on the safety of the most fragile patient.
The improvement proposals and compensatory measures developed in the present study arise from the awareness of the impossibility of intervening in a structural way on the existing architecture. This constraint imposed a reflection oriented towards solutions of an organizational and procedural nature, capable of acting not on the physical configuration of spaces, but on the ways in which they are used daily. In a complex and non-modifiable building context, safety cannot be entrusted to the material transformation of the environment, but rather to the ability of the organization to rethink its processes, redefine operational priorities and introduce compensatory tools suitable to mitigate the critical issues emerged from the analysis of flows. Among the proposals are:
Horizontal signage: a significant role is attributed to the strengthening of horizontal signage. The introduction of a high-contrast color coding, applied directly to the flooring, would allow the creation of real “lanes of movement”, immediately recognizable even in conditions of urgency or high care pressure. This solution, simple but strategic, favors the intuitive respect of assigned pathways and contributes to reducing accidental interferences between flows at different levels of risk, strengthening the organizational readability of spaces;

Checklist dedicated to Flow Hygiene: a further intervention concerns the integration of the current operating room checklists with a section specifically dedicated to flow hygiene. This integration would have the function of systematically monitoring the freedom of transit of corridors, the correct positioning of materials and carts and the respect of areas intended for logistics. The objective is not only to control, but to promote greater organizational awareness: to make visible daily criticalities, often perceived as marginal, and transform them into elements subject to structured verification. In this way, the control of logistical interferences becomes an integral part of the prevention of healthcare-associated infections;

“Protected Corridor” Protocol: in relation to the transport of the transplant patient, the adoption of a defined “protected corridor” protocol is proposed. The procedure provides for the activation of a brief “logistical time-out”, during which the transit of materials and of non-transplant patients along the involved path is temporarily suspended. This measure introduces a temporal separation of flows which, even in the absence of a dedicated structural isolation, allows to reduce the exposure of the immunodepressed patient to potential sources of contamination. It is an intervention with minimal organizational cost, but with high preventive value, capable of transforming a structural limit into an opportunity for conscious regulation of care timing;

Targeted Microclimatic Monitoring: the extension of environmental monitoring to critical points of corridors and areas of intersection between flows is proposed. The increase of particle and microbiological sampling, with particular attention to possible alterations of air flows, would allow early interception of any risk situations not immediately perceptible. In this way, microclimatic surveillance would not remain confined only to operating rooms, but would extend to the pathways that physically translate the care pathway (PDTA), recognizing that transit spaces also represent sensitive environments in the protection of the fragile patient.
In conclusion, the work has highlighted how the prevention of infectious risk in the transplant patient cannot be confined to the strictly clinical dimension, but must include the organization of spaces, the management of time, logistics and the culture of safety. The PDTA does not represent only a tool of therapeutic appropriateness, but a systemic framework within which to place prevention along all phases of the care pathway [17]. In the operating block, the care pathway becomes a physical pathway: corridors, filters, crossings, movements. Every unmanaged interference translates into vulnerability. The study demonstrates that, even in the presence of non-modifiable structural constraints, it is possible to intervene effectively through sustainable organizational measures. The contribution offered by this work, although limited to a specific context, proposes a replicable analysis model, based on the integration between critical reading of care pathways and conscious management of logistical flows, in the perspective of a truly systemic safety.
Bibliography
1. World Health Organization. Global guidelines for the prevention of surgical site infection. Geneva: WHO; 2016.
2. World Health Organization. Guidelines on core components of infection prevention and control programmes. Geneva: WHO; 2016.
3. European Centre for Disease Prevention and Control. Healthcare-associated infections: surgical site infections. Annual epidemiological report. Stockholm: ECDC; 2022.
4. Centers for Disease Control and Prevention. Guideline for the prevention of surgical site infection. Atlanta: CDC; 2017.
5. Ministero della Salute. Piano Nazionale di Contrasto dell’Antimicrobico-Resistenza (PNCAR) 2022–2025. Roma; 2022.
6. Ministero della Salute. Manuale di formazione per il governo clinico: la sicurezza dei pazienti e degli operatori. Roma; 2012.
7. Ministero della Salute. Raccomandazione n. 9: prevenzione delle infezioni del sito chirurgico. Roma; 2008.
8. Società Italiana di Igiene, Medicina Preventiva e Sanità Pubblica. Linee guida per la prevenzione delle infezioni correlate all’assistenza. Roma: SItI; 2019.
9. Istituto Superiore di Sanità. Prevenzione e controllo delle infezioni correlate all’assistenza. Roma: ISS; 2018.
10. European Society for Organ Transplantation. Guidelines for infection management in solid organ transplant recipients. Transplant International. 2019.
11. Fishman JA. Infection in solid-organ transplant recipients. New England Journal of Medicine. 2007;357(25):2601-2614.
12. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection. Infection Control and Hospital Epidemiology. 1999;20(4):250-278.
13. Allegranzi B, Pittet D. Role of hand hygiene in healthcare-associated infection prevention. Journal of Hospital Infection. 2009;73(4):305-315.
14. Associazione Nazionale Medici Direzioni Ospedaliere. Organizzazione e gestione del blocco operatorio. Roma: ANMDO; 2017.
15. Ulrich RS, Zimring C, Zhu X et al. A review of the research literature on evidence-based healthcare design. Health Environments Research & Design Journal. 2008.
16. Joint Commission International. International Patient Safety Goals. Oakbrook Terrace; 2021.
17. Ministero della Salute. Percorsi Diagnostico Terapeutici Assistenziali (PDTA): metodologia e strumenti per l’implementazione. Roma: Ministero della Salute; 2017.